The following are two recent BFR studies that got my attention. Especially the intervention programmes that easily can be implemented in your clinical practise.





Other conditions were BFR has effect.
Physioblog by Andreas Bjerregaard
Physiotherapist, IOC Diploma In Sports Physical Therapy, Certified Mulligan Practitioner, FIFA 11+ instructor and much more.

The following are two recent BFR studies that got my attention. Especially the intervention programmes that easily can be implemented in your clinical practise.
Other conditions were BFR has effect.

Recap
Introduction
The American Academy of Orthopaedic Surgeons (AAOS) released a one-page checklist consisting of patient-specific goals which must be met in order to clear an athlete to RTP following ACLR. These include graft incorporation, graft strength, functional range of motion, stability, strength, functional balance, functional skills, and confidence.
The purpose of the current study is to systematically review the evidence for RTP testing following ACLR, and determine whether it is predictive of re-injuries. Our hypothesis was that there would be a low pass rate in those undergoing RTP testing, but those who passed would have a lower risk of ACL graft rupture
Method
See flow chart.
Results
4.1. Return to play testing
Overall, 34.3% (420/1224) patients passed the RTP testing, with rates ranging between 18.8%88.1%. Those who passed the RTP testing had a statistically significant (47%) decrease in rate of ACL graft re-rupture compared to those who did not pass the RTP testing (RR; 0.53, 95% CI, 0.30–0.93, I2 = 32%, p = 0.03). Encourage to read full text.
4.2. Relationship between return to play testing threshold & subsequent ACL injury
There was a weak positive correlation between a high rate of patients passing the ACL RTP testing in studies and ACL graft rupture rate in those who passed (0.28). There was a weak negative correlation between a high rate of patients passing the ACL RTP testing in studies and contralateral ACL injury rate in those who passed (0.27). There was a strong positive correlation between a high rate of patients passing the ACL RTP testing in studies and ACL graft rupture rate in those who failed (0.80). There was a moderate negative correlation between a high rate of patients passing the ACL RTP testing in studies and contralateral ACL injury rate in those who failed (0.45). There was a weak positive correlation between a high rate of patients passing the ACL RTP testing in studies and total subsequent ACL rupture rate in those who passed (0.01). There was a moderate positive correlation between a high rate of patients passing the ACL RTP testing in studies and total subsequent ACL rupture rate in those who failed (0.63).
Discussion
The most important finding from our study was that passing RTP testing following ACLR results in a lower rate of ACL graft rupture, but not contralateral ACL ruptures. Overall, due to a slightly higher rate of contralateral ACL ruptures, passing
the ACL RTP testing did not lead to a lower rate of subsequent total ACL injury. Additionally, there was a low overall pass rate following current RTP testing measures. Furthermore, a high RTP pass rate (lower threshold for passing) correlated with a
high graft re-rupture rate in the group of patients who had failed RTP testing in those studies. This key finding suggests that a less stringent RTP testing battery may more specifically identify those who are at higher risk of re-tears. Overall, those who passed RTP testing were found to have a lower rate of ACL graft failure by almost a half. Additionally, in all but one study, there was a lower rate of re-injury following passing RTP testing. These findings suggest that RTP tests are a valid tool to screen for potential ipsilateral re-injury.
Conclusion
Our study established that passing RTP testing following ACLR results in a lower rate of ACL graft rupture, but not contralateral ACL injury. Additionally, there is a low overall pass rate following current RTP testing measures. Further refinement
of these criteria may be able to better and more specifically identify those who may be at a high risk of re-injury.

Shaarani et al 2013 reported that a 6 weeks progressive pre-operative rehabilitation for subjects undergoing ACLR led to better single legged hop test and total modified cincinnati scores (a subjective self reported questionnaire asessing symptoms and activity level) at 12 weeks post operatively compared to a group of ACLR subjects whi did not perform pre-rehabilitation. The pre-operative rehabilitation program consisted of 2 supervised gyms session and 2 supercised home sessions per week. The post operative program was stardard for both groups.
Conclusion: The 6-week progressive prehabilitation program for subjects undergoing ACLR led to improved knee function based on the single-legged hop test and self-reported assessment using the modified Cincinnati score. These effects were sustained at 12 weeks postoperatively. This study supports prehabilitation as a consideration for patients awaiting ACLR; however, further studies are warranted.

Running is becoming extremely popular and systematic review found running is associated with 27%, 30%, and 23% reduced lower risk of all cause, cardiovascular and cancer mortality, respectively compared with no running. Significant reduction can be expected for any dose of running, even just once a week or 50 min a week. And here we are not even talking about other health parameters such as mental health.

On the downside, unfortunately there is a large injury rate, it can be anywhere from 15% to 85% in runners all though each studie is representing different definition of running injury and populatiton (Nigg, 2015).

In a prospective study on novice runners, one-third of novice runners stopped running within 6 month due to injury (Nielsen, 2014). One of the most commen injuries among those runners was medial tibial stress fracture, also commonly known as shin splints. However, that diagnose can be very vague and misleading.
To often mixed conditions are the medial tibial stress fracture (MTSS) and tibial stress fracture
When we talk about medial tibial stress fracture, it is a clinical diagnose where the patient describe
In tibial stress fracture its often more focal area of tenderness and less than 5cm radiation. One test to differentiate medial tibial stress fracture (MTSS) and tibial stress fracture could be hop test, as MTSS often can tolerate multiple jump whereas patients with a stress fracture experience severe pain immediately below landing (Kiel and Kaiser, 2018). However, do not base the diagnose solely on the basis of this, then people with severe MTSS may also experience rapid onset pain.
The cause
There are two main theories why it occurs 1. traction of crucal fasciopathy or 2. bone overload.
Predictors
One of the predictors for medial tibial pain in woman is hip weakness. Hip weakness results altered movements that can compromise the ability to protect bone against excessive loads (Verrelst, 2014).
Look out for other diagnose as stress fracturs, chronic exertional compartmental syndrome (CECS), calf injuries (nerve entrapment or vascular pathology) (Reinking, 2007).
PROMS
As clinician we want to know the patient irritability and tthe MTSS score questionnaire is a easy and simply tool to measure it. It is 4 questions and give a score 0-10. Where no symptoms is 0 and 10 is very severe. I can be used once a month to follow progression. The score has been validated by Winters and colleagues. Anecdotally, try to delay running is the score is above 4.
Further more it can be good to collect information about running the last 6 month (days of running / average of km per week, speed session, preferred running distance shoes, foot strike pattern, other sports activities).
Other checklist could be


Imagine
Often it is able to see a bone stress reaction before the person develops pain.
The treatment
The treatment starts with patient education explaining the patient that the shin is sensitive but pain doesnt equal damage. Severity of symptoms is link with tissue overload, not damage. That symptoms can settle soon, but it can take a very long time to get back to pre-injury level and finally that set backs and flare up is very commonly during recovery.
According to Mulvad, 2018, that average recovery time is 70 days.
The main concepts of the training is
Podcast:
Danish: https://www.sportsfysioterapi.dk/fagligt/podcast/
English: https://www.running-physio.com/rtr/
English: healthywealthysmart 528: DR. ELLIE SOMERS: BONE STRESS INJURY & REHAB IN FEMALE RUNNERS
More about bone stress see here (Clinical update on Bone Stress Injuries and Femoral Neck Stress Fracture. Can MRI Grade Help Predict Return-to-Running Time?, Ramey LN et al., Am J Sports Med.(2016) Preview
Reference

WHAT IS ALREADY KNOWN ON THIS TOPIC
Several non-randomised studies have suggested that for patients with rupture of the anterior cruciate ligament (ACL), clinical results for early reconstruction of the ACL compared with rehabilitation alone are similar Evidence from randomised controlled trials is lacking The preferred treatment for rupture of the ACL (surgery or rehabilitation) is unclear.
WHAT THIS STUDY ADDS
Patients who underwent early surgical reconstruction of the ACL, compared with those who had rehabilitation followed by elective surgical reconstruction, had improved perceptions of symptoms, knee function, and ability to participate in sports at the two year follow-up This finding was significant but the clinical importance is unclear Interpretation of the results of the study should consider that 50% of patients randomised to the rehabilitation group did not need surgical reconstruction.
The aim
The aim of the trial was to assess whether a clinically relevant difference existed in patients’ perceptions of symptoms, knee function, and ability to participate in sporting activities between two commonly used treatment regimens: early reconstruction of the ACL versus rehabilitation and optional delayed ACL reconstruction. The primary outcome was measured with the International Knee Documentation Committee score over a period of two years after rupture of the ACL.
Early ACL reconstruction
Arthroscopic reconstruction of the ACL was scheduled within six weeks after randomisation. Surgeons chose their preferred technique and graft, and decided if more intra-articular surgery was necessary.
Rehabilitation with optional delayed ACL reconstruction
For non-operative treatment, patients were referred to a physical therapist for a supervised physical therapy programme for a minimum of three months, according to the recommendations of the Dutch ACL guideline.1 After a minimum of three months of rehabilitation, patients could opt for reconstruction of the ACL if instability persisted or if the desired activity level was not reached.
Questionnaire answer
Patients were seen at the outpatient clinic at baseline, and at 12 and 24 months. Patients completed a questionnaire at three, six, and nine months after randomisation. All questionnaires were completed digitally





Conclusions
In patients with acute rupture of the ACL, those who underwent surgical reconstruction alone,
compared with rehabilitation and optional surgical reconstruction, had improved perceptions of
symptoms, knee function, and ability to participate in sports at the two year follow-up. This finding was significant (P=0.026) but the clinical importance is unclear. Interpretation of the results of the study should consider that 50% of the patients randomised to the rehabilitation group did not need surgical reconstruction.
To cite: Kotsifaki A, Whiteley R, Van
Rossom S, et al. Br J doi:10.1136/ bjsports-2020-103677

INTRODUCTION
Functional hop testing is traditionally used to determine readiness to return to sport (RTS) after anterior cruciate ligament reconstruction (ACLR).1 2 Typically, functional symmetry between legs is assessedwith a hop test battery The primary hop tests are in forward direction and the outcome of interest is distance in three of them—single hop, triple hop and cross-over hop for distance.5 With these tests, Limb Symmetry Index (LSI) of >90% in distance hopped is recommended as a cut-off point for safe RTS.
The work done during the propulsion phase of the hop then needs to be absorbed by the same limb during the landing phase. Examining the work during propulsion and landing, as well as the contribution of the different joints may reveal motor strategies associated with aberrantly high, potentially injurious, loads. The relative contributions of each part of the kinetic chain likely vary depending on the individual’s motor strategy. Protectively off-loading one joint might result in higher compensatory loading at another.
This article tried to describe depth the biomechanical performance (kinematics, kinetics, work, and individual muscle forces) of athletes at the time they had met all criteria for RTS and compare with healthy controls during the propulsion and landing phases of the SLHD. The objective of this study was to evaluate biomechanical components during the propulsion and landing phases of the SLHD test in athletes with ACLR who had passed criteria for RTS, compared with contralateral knees and uninjured athletes.
Participants, inclusion and exclusion criteria
49 male participants was included in this study, 26 eligible patients after primary ACLR and 23 control subjects The RTS process employs a shared decision making strategy18 which includes consideration of key RTS criteria including (1) clearance by both their surgeon and physiotherapist, (2) completion of a sports specific on-field Rehabilitation programme, (3) quadriceps strength LSI>90%, and (4) hop test battery LSI>90%0.4 ACLR individuals were athletes (preinjury Tegner score ≥7) aged between 18 and 35 years with a complete, unilateral ACL injury, either with an autologous ipsilateral bone-patellar-tendon-bone or a hamstrings graft (semitendinosus and gracilis) as clinically decided by the treating surgeon and athlete. Subjects with concomitant meniscal injury that did not significantly impede the rehabilitation course were also included in the study. Participants were excluded if they had concomitant grade III knee ligament injury (other than ACL), full thickness articular cartilage lesion, history of other lower extremity surgery (in either leg), back pain or lower extremity injury (other than primary ACL) in the prior 3 months.
DISCUSSION
Despite passing strict testing criteria to RTS, differences in biomechanics were identified between the injured and uninjured limbs of athletes after ACLR, as well as with the healthy comparison group.
Hop distance as a metric of knee function needs reappraisal
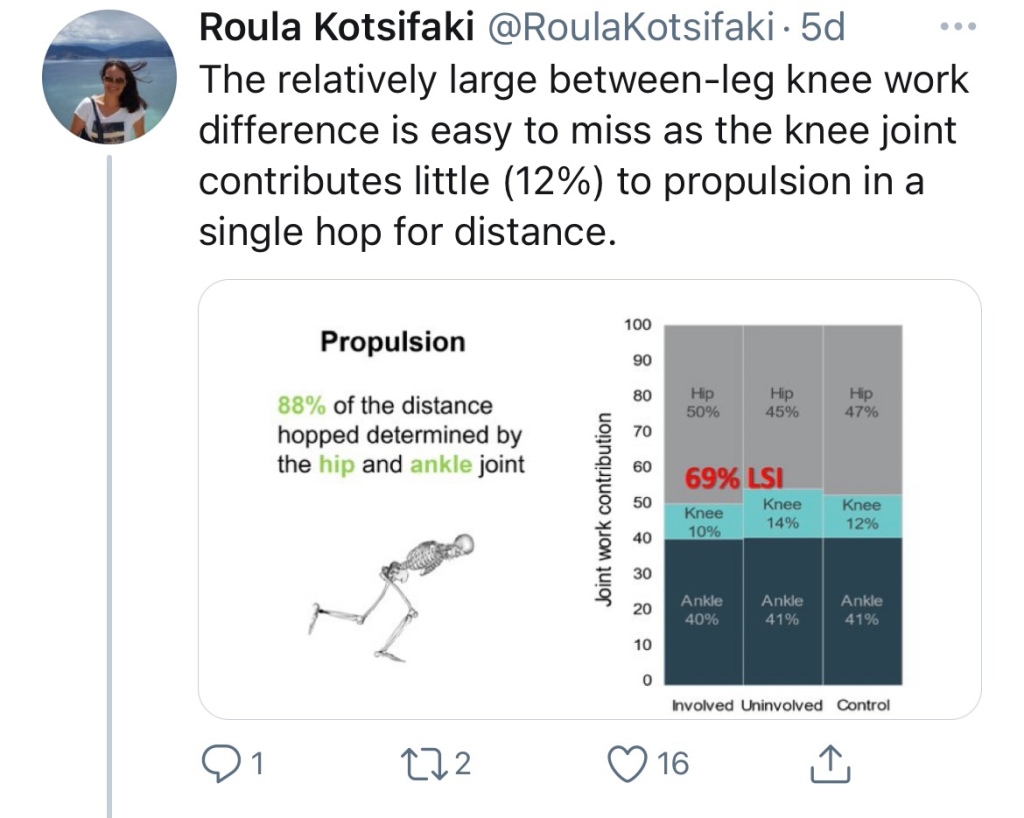
Athletes after ACLR were almost symmetrical in terms of hop distance (97%), but they still exhibited moderate to large differences in knee function. The ACLR group achieved 69% symmetry in knee work done during propulsion. This relatively large between-leg difference is more easily understood when we recognise that the knee joint contributes little (about 12%) to the propulsive phase of a SLHD. With 88% of the distance hopped being determined by the hip and ankle joint, deficits at the knee joint are easily missed. Simply put: the distance hopped is a poor measure of knee joint function, and largely reflects hip and ankle function. Consequently, it may not be the appropriate metric to use for testing an athlete with a knee injury and its relevance is questionable.



Clinical implications
Hop distance symmetry is commonly used as a criterion for an athlete to RTS after ACLR. The results of this study indicate that during a SLHD, symmetry in hop distance does not ensure symmetry in lower limb biomechanical parameters, especially for the knee joint. Future research might explore if these results can be generalised to the other common tests like the triple hop and the cross-over hop for distance and whether they measure similar constructs. Measuring hop distance, or its symmetry, risks overestimating rehabilitation status in terms of the knee joint, may lead to erroneous progression, and offers little additional clinical information in the RTS-readiness decision. Conversely, the SLHD task, and specifically the landing phase, can offer valuable information on the status of the knee joint, but requires three-dimensional biomechanical analysis—an apparatus not frequently available in clinical setting. Consequently, future research should focus on identifying proxy variables of these loading measures, perhaps from wearable technology or other approaches, which would allow monitoring these parameters in a clinical setting. In the absence of this technology, we suggest tasks other than SLHD, and variables other than hop distance may be more appropriate to capture the differences between legs and offer a more accurate estimation of the status of the knee.
CONCLUSION
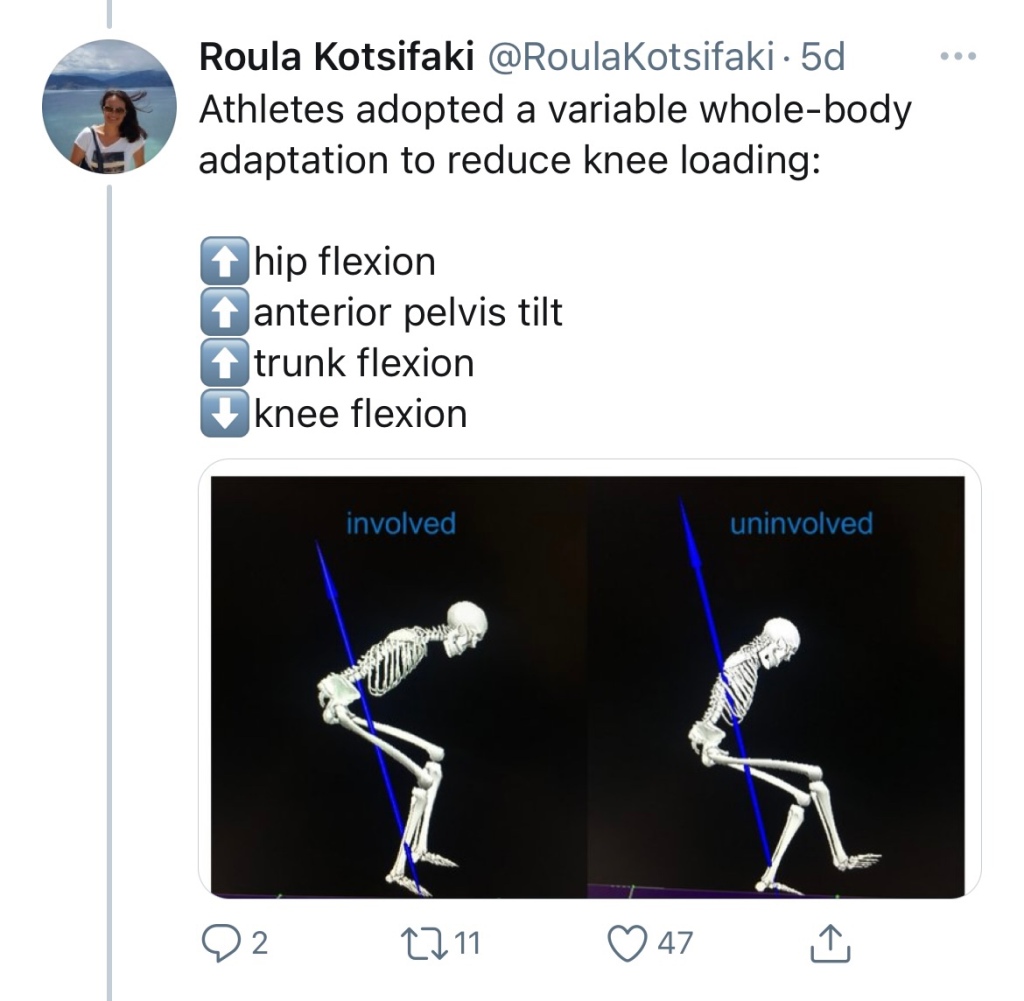
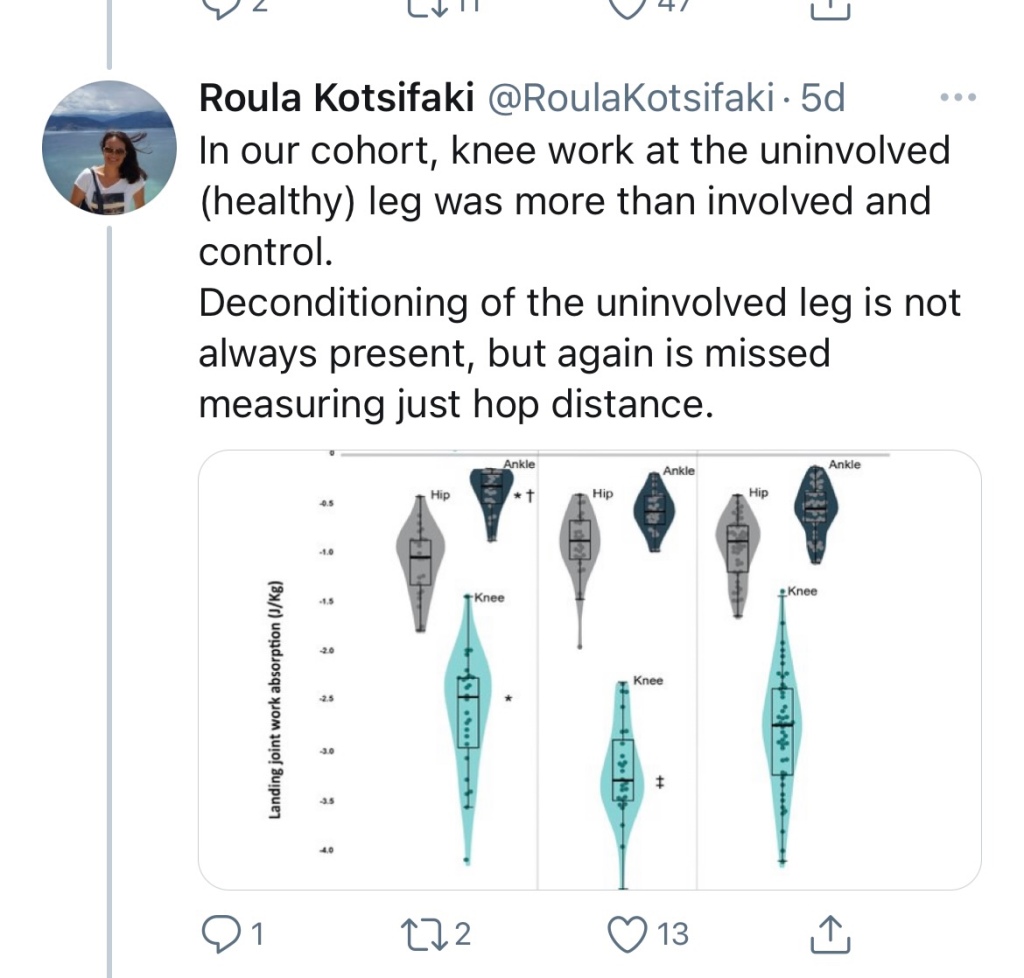
Symmetry in performance of single leg hop distance masks important deficits in knee joint work in male athletes after ACLR. Specifically, they appear to underload their reconstructed knee during landing (while compensating at their hip) and overload their uninjured knee compared with healthy controls.





Just finished 3 month Bill Star program

4-2-2021 3RM 65.8kg
FCN søger ny fysioterapeut til U19 hold.
Jeg har i mange år været imponeret af FCN medicinske setup, som udefra set virker til at være et af de bedst i Danmark.
En af de store udfordringer som fysioterapeut i en klub er at få spillere til at “købe ind” på den behandling, de forebyggelsesprogrammer, og den performance optimering der bliver givet, så spillerne ikke søger ukoordineret behandling andre steder.Flere undersøgelser fra UEFA har peget på at succes blandt andet afhænger af hvor mange spiller klubben har til rådighed, og at de klubber med over 86% spiller rådighed i løbet af sæsonen, har større chance for at vinde mesterskaber end klubber med mange skader (1, 2). Derudover viser det at intern kommunikation og ledelsesstil også påvirker skades incidensen (3, 4) Derfor vil et godt velbetalte behandlingsteam med erfaring, efteruddannelse, der kan nedsætte “fraværsdage” og potentiale fraværsdage (skadesforebyggelse) være en god return of investment for klubben (5).
Derfor, er jeg også ellevild med den standard FCN fastsætter til deres behandlere på u19, når jeg ser andre elite fodboldklubber fuldtidsansætte nyuddannede fysioterapeuter for landets bedste fodboldtalenter. Når det er sagt, så var jeg så heldig selv at få arbejde i 1. divisionen som 2 års fysioterapeutstuderende og sad med ved kampene. Det var en kæmpe oplevelse og virkelig lærerigt, men set i bakspejlet, så var det nok ikke den mest ansvarlige, at min lærdom skete i et elitemiljø ved at gamble med akutte hjernerystelser, muskelskader eller til dagligt være med i beslutningsprocessen omkring retur til sport.
Jeg håber, at dette jobopslag kan være med til at sætte standarden for den kvalitetsikring der burde være i elitemiljøet, så spillere og evt. forældre trygt kan stole på de hænder tager fandt om deres talentfulde ben. Hvis du er interesseret i at blive idrætsfysioterapeut, så en varm anbefaling til at søge denne position.
Andreas
1) Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study https://bjsm.bmj.com/content/47/12/738
2) Does player unavailability affect football teams’ match physical outputs? A two-season study of the UEFA champions league https://www.sciencedirect.com/…/pii/S1440244017309957….
3) Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs https://bjsm.bmj.com/content/53/5/304
4) Is there a correlation between coaches’ leadership styles and injuries in elite football teams? A study of 36 elite teams in 17 countries https://bjsm.bmj.com/content/52/8/527
5) Preventing injuries in professional football: thinking bigger and working together https://bjsm.bmj.com/content/50/12/709
Læs også Er du bedre end en Ørn?
Presentation for Journal Club in Aspetar Hospital December 2020
Online ACL rehab
Making the most of social media to learn, share and influence. Tweetchats on third Monday of month at 20.00 GMT
Simple, practical, honest advice
Indikationer, kontraindikationer, klinisk ræsonnering og forskning
Physiotherapist, IOC Diploma In Sports Physical Therapy, Certified Mulligan Practitioner, FIFA 11+ instructor and much more.
The latest news on WordPress.com and the WordPress community.
